If current laws remained generally unchanged, the United States would face steadily increasing federal budget deficits and debt over the next 30 years—reaching the highest level of debt relative to GDP ever experienced in this country.The full CBO Report, "The 2017 Long-Term Budget Outlook" follows:
Source: CBO
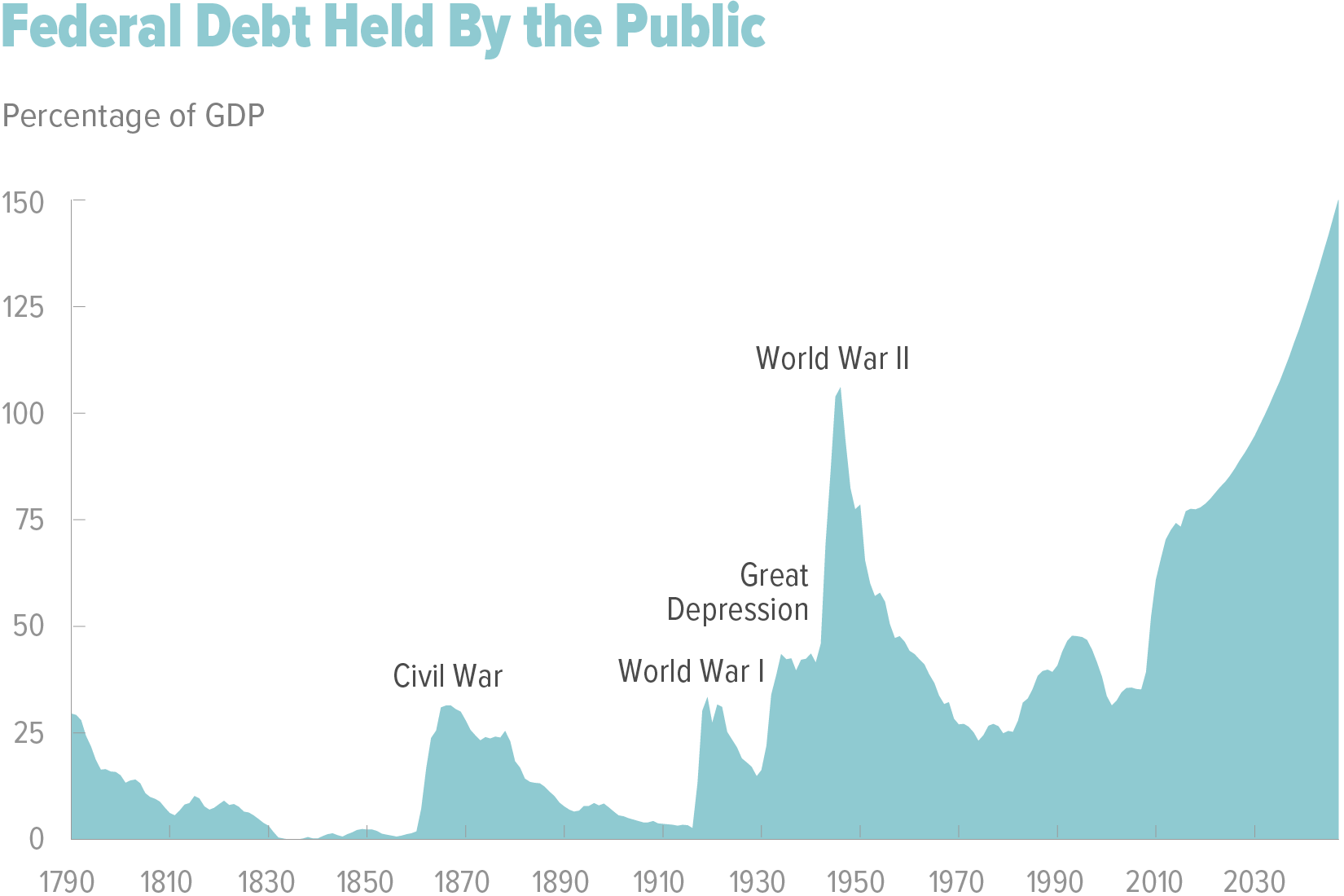
At 77 percent of gross domestic product (GDP), federal debt held by the public is now at its highest level since shortly after World War II. If current laws generally remained unchanged, the Congressional Budget Office projects, growing budget deficits would boost that debt sharply over the next 30 years; it would reach 150 percent of GDP in 2047. The prospect of such large and growing debt poses substantial risks for the nation and presents policymakers with significant challenges.
Why Are Projected Deficits Rising?
In CBO’s projections, deficits rise over the next three decades—from 2.9 percent of GDP in 2017 to 9.8 percent in 2047—because spending growth is projected to outpace growth in revenues (see figure below). In particular, spending as a share of GDP increases for Social Security, the major health care programs (primarily Medicare), and interest on the government’s debt.
Source: CBO
Much of the spending growth for Social Security and Medicare results from the aging of the population: As members of the baby-boom generation age and as life expectancy continues to increase, the percentage of the population age 65 or older will grow sharply, boosting the number of beneficiaries of those programs.
In addition, growth in spending on Medicare and the other major health care programs is driven by rising health care costs per person, which are projected to increase more quickly than GDP per capita (after the effects of aging and other demographic changes are removed). CBO projects that those health care costs will rise—although more slowly than they have in the past—in part because of the effects of new medical technologies and rising personal income.
The federal government’s net interest costs are projected to rise sharply as a percentage of GDP for two main reasons. The first and more important is that interest rates are expected to rise from their current low levels, making any given amount of debt more costly to finance. The second reason is the projected increase in deficits: The larger they are, the more the government will need to borrow.
*** What Might the Consequences Be If Current Laws Remained Unchanged?
Large and growing federal debt over the coming decades would hurt the economy and constrain future budget policy. The amount of debt that is projected under the extended baseline would reduce national saving and income in the long term; increase the government’s interest costs, putting more pressure on the rest of the budget; limit lawmakers’ ability to respond to unforeseen events; and increase the likelihood of a fiscal crisis, an occurrence in which investors become unwilling to finance a government’s borrowing unless they are compensated with very high interest rates.

The 2017 Long-Term Budget Outlook - CBO on Scribd